The Democratic Republic of Congo has confirmed a new Ebola outbreak in its eastern Ituri province that has already claimed 80 lives out of 246 suspected cases. While standard news wires report these numbers as a routine resurgence of a familiar enemy, the medical reality on the ground is far more dangerous. This is not the standard Ebola virus the international community has spent a decade preparing for. Health Minister Samuel Roger Kamba Mulamba confirmed that laboratory testing has identified the culprit as the Bundibugyo strain, a rare variant for which there are zero approved vaccines or therapeutic treatments.
The crisis crossed an international border almost immediately, with Uganda confirming a fatal, imported case in Kampala linked to the Congolese outbreak. This rapid transmission exposes a terrifying convergence of a vulnerable viral mutation, mining-driven migration, and active militia warfare that threatens to render traditional containment strategies entirely useless.
The Illusion of Preparedness
For the past several years, global health agencies have pointed to the Democratic Republic of Congo (DRC) as a success story in outbreak management. After battling 16 prior outbreaks, local medical teams became highly proficient at deploying the Ervebo vaccine, administering monoclonal antibodies, and spinning up mobile testing labs.
That playbook has been rendered obsolete in Ituri.
The international community's stockpile of medical countermeasures is almost exclusively engineered to fight the Ebola Zaire strain. When the Zaire strain strikes, health workers implement ring vaccination, inoculating every contact of an infected person to create a human shield against the virus. Against the Bundibugyo strain, that shield does not exist.
Ebola Strains and Medical Readiness:
+-------------------+-----------------------+--------------------------+
| Virus Strain | Historic Fatality Rate| Approved Vaccine Status |
+-------------------+-----------------------+--------------------------+
| Zaire Ebolavirus | 60% - 90% | Fully Stockpiled (Ervebo)|
| Bundibugyo Strain | 36% - 40% | Zero Approved Vaccines |
+-------------------+-----------------------+--------------------------+
While the Bundibugyo strain has historically exhibited a lower case-fatality rate than its Zaire cousin, relying on that historical data is a dangerous gamble. The virus is currently ripping through the dense urban and mining environments of Mongwalu, Rwampara, and the provincial capital of Bunia. Without a vaccine to halt transmission, containment relies purely on the oldest, most grueling methods of medicine: strict isolation, manual contact tracing, and flawless barrier nursing.
How Gold and Guns Fuel the Transmission Vector
The epicenter of this outbreak is not a isolated village cut off from civilization. It is a highly mobile, volatile economic hub.
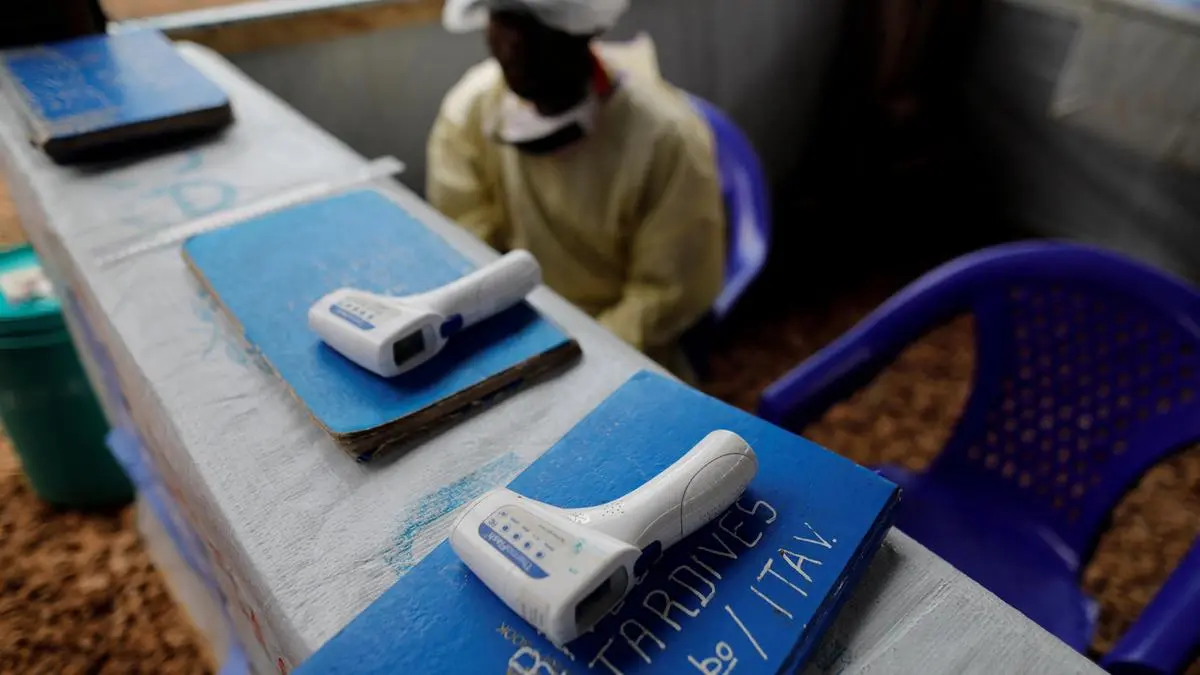
The suspected index case—a nurse who died at the Evangelical Medical Centre in Bunia after exhibiting severe fever, vomiting, and internal bleeding—revealed just how deeply the disease has already penetrated the local healthcare infrastructure. In eastern DRC, formal hospitals are few, and informal, under-resourced clinics are the frontline defense. When a health worker dies, it usually means dozens of patients have already been exposed via contaminated needles or lack of personal protective equipment.
More concerning is the role of the region's artisanal gold mines. Ituri's informal mining sector attracts thousands of migrant laborers who move constantly across fluid provincial lines and poorly monitored borders.
- High Mobility: Miners move from deep forest excavation sites to crowded urban trade markets within days.
- Border Proximity: Bunia sits dangerously close to the porous frontiers of Uganda and South Sudan.
- Shadow Economies: Much of the movement occurs outside formal border checkpoints, making traditional health screenings impossible to enforce.
Compounding this logistical nightmare is an active humanitarian disaster. Ituri is currently engulfed in violent territorial clashes between rival ethnic militias and rebel groups, including the M23 movement and the Allied Democratic Forces (ADF). Militant activity has displaced hundreds of thousands of civilians into squalid, overcrowded encampments where sanitation is nonexistent.
When a militia attacks a village, contact tracing stops dead. Epidemiologists cannot track exposed individuals who have fled into the bush or crossed into neighboring nations to escape a machete or a bullet. Medical teams trying to reach remote health zones face the very real threat of ambush.
The Failure of Early Warning Systems
The World Health Organization admitted it learned of suspected hemorrhagic fever cases in Ituri on May 5 and dispatched an investigation team. However, initial field samples tested negative. It took nearly ten days for a laboratory in Kinshasa to override those early results and confirm the positive cases.
That ten-day blind spot allowed the virus to spread unchecked through local communities.
The initial false negatives point to a systemic vulnerability in field diagnostics. Standard rapid diagnostic tests used in remote African clinics are heavily optimized for the Zaire strain. When confronted with the genetic variance of Bundibugyo, these tests can yield weak or entirely negative results if the viral load in the patient's blood is not yet peaking.
By the time centralized PCR testing in Kinshasa finally sounded the alarm, the virus had already boarded cross-border transit. The confirmed casualty in Uganda—a Congolese national who spent three days in a Kampala hospital before dying—illustrates how quickly a localized flare-up can become an international emergency. Uganda has quarantined all known contacts, but the delay in diagnosis means the virus had ample opportunity to seed secondary chains of transmission along the transit corridors.
What the Ground Reality Demands
International donors routinely treat Ebola as a discrete medical emergency that can be solved by flying in field tents and foreign specialists. That approach will fail in Ituri.
The World Health Organization has released $500,000 from its contingency fund, but cash alone cannot buy security or build roads in a war zone. If the international community wants to prevent this Bundibugyo outbreak from mirroring the catastrophic 2014 West African epidemic, the strategy must pivot immediately.
First, the response requires direct integration with UN peacekeeping assets to provide armed escorts for medical personnel. Health workers cannot fight a deadly pathogen while looking over their shoulders for rebel factions.
Second, diagnostic priorities must shift. Rather than relying on centralized laboratories located over 600 miles away in Kinshasa, gene-sequencing and specialized PCR equipment capable of identifying non-Zaire strains must be deployed directly to border towns like Bunia and regional hubs in Uganda.
The window to contain this virus within the eastern Congo is rapidly closing. If the mining networks and displacement camps of Ituri become permanent vectors for an untreatable strain of Ebola, the regional fallout will be measured in thousands of lives, not dozens. Containment requires clearing the logistical and security bottlenecks now, before the virus moves faster than the bureaucracy trying to track it.